An accurate diagnosis of NMOSD is critical, as patients with NMOSD have been misdiagnosed with MS1
Differential diagnosis of Neuromyelitis Optica Spectrum Disorder (NMOSD) from multiple sclerosis (MS) is important to individualize treatment.1-3

MISDIAGNOSIS
NMOSD PATIENTS MAY BE HIDDEN WITHIN THE MS POPULATION
In a retrospective study of patients with NMOSD, 42.5% (31/73) with available data were initially misdiagnosed with MS. The wrong diagnosis of MS became less common after aquaporin-4 immunoglobulin G (AQP4-IgG) testing became commercially available in 2005 (20% vs 54.2% before 2005; P<0.007)1*
*Retrospective study based on the German Neuromyelitis Optica Study Group (NEMOS) registry of 175 patients with NMOSD and known AQP4 antibody status; an expert panel of NEMOS members reviewed all cases from August 2009 to August 2011.1SHARED SYMPTOMS
LOOK BEYOND SHARED SYMPTOMATOLOGY TO DIFFERENTIATE NMOSD FROM MS
| Disease impact | NMOSD4-7 | MS8 |
|---|---|---|
| Vision loss | ||
| Blindness | ||
| Spasms | ||
| Limb weakness | ||
| Sensation loss | ||
| Paralysis | ||
| Loss of bowel/bladder function | ||
| Hiccups | ||
| Nausea | ||
| Vomiting |
Impact due to lesions in the area postrema.9
AQP4-IgG antibodies are present in 73% of NMOSD cases but are not present in MS.10
DIFFERENCES
NMOSD AND MS DIFFER IN MANY IMPORTANT AREAS
Primary site of damage
NMOSD primarily targets astrocytes while MS primarily targets oligodendrocytes and myelin.11
The role of complement
Unlike MS, damage in NMOSD is complement-mediated.3,11
Relapse recovery
Compared to MS, relapse recovery is poorer in NMOSD, with patients being less likely to return to baseline.12
Relapse-dependent disability
While in MS, disability is largely independent of relapses, in NMOSD, relapses directly lead to cumulative disability.3
Median age of onset
In MS, the median age of onset is 29 years, whereas it’s 39 years in NMOSD.4
Female to male ratio
The female to male ratio in MS is 2:1, but in NMOSD the ratio is 9:1.4
MISDIAGNOSIS
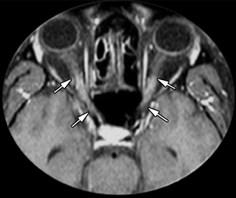
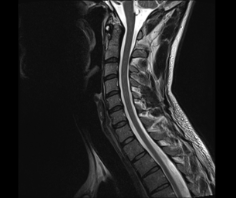
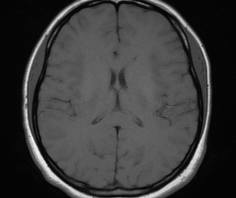
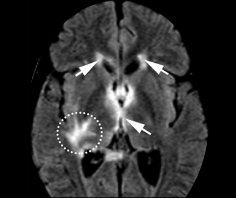
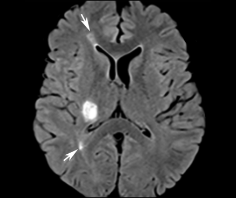
MRI EVIDENCE POINTS TO IMPORTANT DIFFERENTIATORS BETWEEN NMOSD AND MS LESIONS
Normal
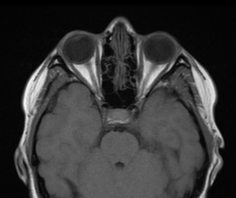
NMOSD
MS

Normal
NMOSD

MS

Normal
NMOSD
MS
References: 1. Jarius S, Ruprecht K, Wildemann B, et al. Contrasting disease patterns in seropositive and seronegative neuromyelitis optica: a multicentre study of 175 patients. J Neuroinflammation. 2012;9:14. 2. Mealy MA, Mossburg SE, Kim SH, et al. Long-term disability in neuromyelitis optica spectrum disorder with a history of myelitis is associated with age at onset, delay in diagnosis/preventive treatment, MRI lesion length and presence of symptomatic brain lesions. Mult Scler Relat Disord. 2019;28:64-68. 3. Kim SM, Kim SJ, Lee JH, Kuroda H, Palace J, Fujihara K. Differential diagnosis of neuromyelitis optica spectrum disorders. Ther Adv Neurol Disord. 2017;10(7):265-289. 4. Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol. 2007;6(9):805-815. 5. Hinson SR, Lennon VA, Pittock SJ. Autoimmune AQP4 channelopathies and neuromyelitis optica spectrum disorders. Handb Clin Neurol. 2016;133:377-403. 6. Pereira WL, Reiche EM, Kallaur AP, Kaimen-Maciel DR. Epidemiological, clinical, and immunological characteristics of neuromyelitis optica: a review. J Neurol Sci. 2015;355(1-2):7-17. 7. Mutch K, Methley A, Moore P, Jacob A. Life on hold: the experience of living with neuromyelitis optica. Disabil Rehabil. 2014;36(13):1100-1107. 8. Ghasemi N, Razabi S, Nikzad E. Multiple sclerosis: pathogenesis, symptoms, diagnoses and cell-based therapy. Cell J. 2017;19(1):1-10. 9. Wingerchuk DM, Banwell B, Bennett JL, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology. 2015;85(2):177-189. 10. Hamid SHM, Whittam D, Mutch K, et al. What proportion of AQP4-IgG-negative NMO spectrum disorder patients are MOG-IgG positive? A cross sectional study of 132 patients. J Neurol. 2017;264(10):2088-2094. 11. Kawachi I, Lassmann H. Neurodegeneration in multiple sclerosis and neuromyelitis optica. J Neurol Neurosurg Psychiatry. 2017;88(2):137-145. 12. Masuda H, Mori M, Uzawa A, et al. Recovery from optic neuritis attack in neuromyelitis optica spectrum disorder and multiple sclerosis. J Neurol Sci. 2016;367:375-379. 13. Gaillard F. Normal brain (MRI). Radiopaedia website. https://radiopaedia.org/cases/normal-brain-mri-6?lang=us. Accessed April 10, 2019. 14. Dutra BG, da Rocha AJ, Nunes RH, Maia ACM. Neuromyelitis optica spectrum disorders: spectrum of MR imaging findings and their differential diagnosis. Radiographics. 2018;38(1):169-193. 15. Di Muzio B. Normal cervical spine MRI. Radiopaedia website. https://radiopaedia.org/cases/normal-cervical-spine-mri-1?lang. Accessed April 10, 2019.


